
Super P-Force
"Order super p-force 160 mg otc, erectile dysfunction treatment in urdu."
By: Neal H Cohen, MD, MS, MPH
- Professor, Department of Anesthesia and Perioperative Care, University of California, San Francisco, School of Medicine, San Francisco, California

https://profiles.ucsf.edu/neal.cohen
Protective sensation: 10-g monofilament these tests not only screen for the presence of dysfunction but also predict future risk of complications erectile dysfunction high blood pressure discount 160mg super p-force otc. See American Diabetes Association position statement "Diabetic Neuropathy" for more details (99) erectile dysfunction ugly wife buy super p-force 160 mg on-line. The early recognition and appropriate management of neuropathy in the patient with diabetes is important erectile dysfunction treatment scams cheap super p-force 160mg on-line. Nondiabetic neuropathies may be present in patients with diabetes and may be treatable erectile dysfunction latest medicine proven 160mg super p-force. Recognition and treatment of autonomic neuropathy may improve symptoms, reduce sequelae, and improve quality of life. Specific treatment for the underlying nerve damage, other than improved glycemic control, is currently not available. Glycemic Screening c All patients should be assessed for diabetic peripheral neuropathy S112 Microvascular Complications and Foot Care Diabetes Care Volume 41, Supplement 1, January 2018 Diabetic Autonomic Neuropathy the symptoms and signs of autonomic neuropathy should be elicited carefully during the history and physical examination. Major clinical manifestations of diabetic autonomic neuropathy include hypoglycemia unawareness, resting tachycardia, orthostatic hypotension, gastroparesis, constipation, diarrhea, fecal incontinence, erectile dysfunction, neurogenic bladder, and sudomotor dysfunction with either increased or decreased sweating. Gastrointestinal neuropathies may involve any portion of the gastrointestinal tract with manifestations including esophageal dysmotility, gastroparesis, constipation, diarrhea, and fecal incontinence. Gastroparesis should be suspected in individuals with erratic glycemic control or with upper gastrointestinal symptoms without another identified cause. Diabetic autonomic neuropathy may also cause genitourinary disturbances, including sexual dysfunction and bladder dysfunction. Female sexual dysfunction occurs more frequently in those with diabetes and presents as decreased sexual desire, increased pain during intercourse, decreased sexual arousal, and inadequate lubrication (103). Although the evidence for the benefit of near-normal glycemic control is not as strong for type 2 diabetes, some studies have demonstrated a modest slowing of progression without reversal of neuronal loss (30,108). In longer-term studies, a small increase in A1C was reported in people with diabetes treated with duloxetine compared with placebo (124). Adverse events may be more severe in older people, but may be attenuated with lower doses and slower titrations of duloxetine. The therapeutic goal is to minimize postural symptoms rather than to restore normotension. Dietary changes may be useful, such as eating multiple small meals and decreasing dietary fat and fiber intake. B the examination should include inspection of the skin, assessment of foot deformities, neurological assessment (10-g monofilament testing with at least one other assessment: pinprick, temperature, vibration), and vascular assessment including pulses in the legs and feet. C A multidisciplinary approach is recommended for individuals with foot ulcers and high-risk feet (e. B Refer patients who smoke or who have histories of prior lower-extremity complications, loss of protective sensation, structural abnormalities, or peripheral arterial disease to foot care specialists for ongoing preventive care and life-long surveillance. B the use of specialized therapeutic footwear is recommended for highrisk patients with diabetes including those with severe neuropathy, foot deformities, or history of amputation. To assess risk, clinicians should ask about history of foot ulcers or amputation, neuropathic and peripheral vascular symptoms, impaired vision, renal disease, tobacco use, and foot care practices. However, patients should be provided adequate information to aid in selection of appropriate footwear. Most diabetic foot infections are polymicrobial, with aerobic gram-positive cocci. Wounds without evidence of soft tissue or bone infection do not require antibiotic therapy. Renal insufficiency in the absence of albuminuria and retinopathy among adults with type 2 diabetes mellitus. Acute kidney injury episodes and chronic kidney disease risk in diabetes mellitus.
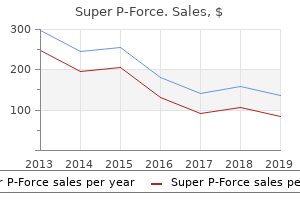
The rate corresponding to erectile dysfunction under 25 super p-force 160mg overnight delivery the rightmost pathway (Asbestos ) is 58-11 = 47/100 erectile dysfunction za generic 160 mg super p-force amex,000 py erectile dysfunction circumcision order 160 mg super p-force with visa. The rate that corresponds to erectile dysfunction causes psychological generic 160 mg super p-force fast delivery the third causal pathway (Smk Asb ) is now reduced since some of cases with both exposures could be due to the effect of asbestos. So the rate that corresponds to the third pathway is now (602-112-11-47)/100,000 py = 410/100,000 py. We might take these rates and reason as follows: Increase due to smoking Increase due to asbestos Total increase expected due to both Total observed increase 123 - 11 = 112 58 - 11 = 47 112 + 47 = 159 602 - 11 = 591! Since the increase due to the combined effect greatly exceeds that expected from our (additive) model, we would conclude that the effect is synergistic. Alternatively, we might reason in relative terms: Relative increase due to smoking Relative increase due to asbestos Total increase expected due to both Total observed increase 123 / 11 = 11. We are thus faced with a situation where the decision about effect modification depends upon what model we employ to arrive at an expected joint effect to compare with the observed joint effect (or equivalently, upon the scale of measurement, hence the term "effect measure modification"). Before pondering this dilemma further, we should first state the additive and multiplicative models explicitly. To do so we introduce a notation in which "1" indicates presence of a factor, a "0" indicates absence of a factor, the first subscript represents the first risk factor, and the second subscript represents the second risk factor (see below). The first subscript indicates presence or absence of the first factor; the second subscript, presence or absence of the second factor. For example, R10 refers to the rate for persons exposed to the first factor but not to the second. That rate can be referred to as the rate for the exposed (to factor 1) in the stratum without factor 2; equivalently, R10 can be referred to as the rate for the unexposed (to factor 2) in the stratum where factor 1 is present. In contrast, a single subscript (R1) means the factor is present, with other factors present or not present (i. Additive model Under an additive model, the increase in rate or risk from a combination of factors equals the sum of the increases from each factor by itself. We can express this statement algebraically, using the rate (or risk) difference: The additive model, expressed in terms of excess risk, is therefore: Excess risk for A and B together = Excess risk for A + Excess risk for B i. With this expression we can evaluate the additive model even from case-control data. The reason that we need to subtract the baseline risk in the last of these forms is that risk in the presence of any of the factors includes, necessarily, the ever-present background risk. So when we add the risk for one factor to the risk for another factor, the background risk is added twice. Thus, when we refer to Rijk as the risk (or rate) for a factor "by itself", the "by itself" really means "with no other specified factors", since the baseline risk is, by definition, always present. As before, "by itself" means without other specified factors, but including baseline risk. To see this, use the additive and multiplicative models just presented with the data in the above table to fill in the rightmost two columns of the following table. The multiplicative model says that the rate for any combination of the three factors (with cutpoints defined as in the table) equals the product of the rates for each of the three factors when neither of the other two is present, divided by the square of the rate for those who have none of the three factors (i. The better fit for the The "natural" scaling the additive model has been put forth by Rothman as the "natural" scaling.
Buy super p-force 160 mg on line. Laboob-e-Kabir | Mardana Taqat Aur Timing Ka Zabardast Nuskha Wasib Dawakhana By My Help in Health.
Asthma and Latino Cultures: Different Prevalence Reported Among Groups Sharing the Same Environment which antihypertensive causes erectile dysfunction super p-force 160mg fast delivery. Lower Bronchodilator Responsiveness in Puerto Rican than in Mexican Subjects with Asthma erectile dysfunction drug mechanism purchase 160 mg super p-force otc. Elevated Asthma in Indoor Environmental Exposures Among Puerto Rican Children of East Harlem erectile dysfunction or gay 160mg super p-force sale. Quickstats: Percentage Distribution of Hospitalizations for Types of Respiratory Diseases Among Children Aged <15 Years - National Hospital Discharge Survey erectile dysfunction at 65 order super p-force 160 mg on-line, United States, 2005. National Ambulatory Medical Care Survey and National Hospital Ambulatory Medical Care Survey, 2005. The Effects of Race/Ethnicity and Income on Early Childhood Asthma Prevalence and Health Care Use. National Asthma Education and Prevention Program Expert Panel Report 3: Guidelines for the Diagnosis and Management of Asthma. Use of Asthma Guidelines by Primary Care Providers to Reduce Hospitalizations and Emergency Department Visits in Poor, Minority, Urban Children. Benefit from the Inclusion of Self-treatment Guidelines to a Self-management Programme for Adults with Asthma. Effect of Education Programs on Asthma Control and Quality of Life in Adult Asthma Patients. Bronchiolitis to Asthma: A Review and Call for Studies of Gene-Virus Interactions in Asthma Causation. Associations Between Outdoor Air Pollution and Childhood Asthma Symptoms in Metropolitan Areas, United States. Randomized Comparison of Strategies for Reducing Treatment in Mild Persistent Asthma. Air & Radiation: Six Common Pollutants; Particulate Matter, Health and Environment. American Thoracic Society/ European Respiratory Society Statement: Standards for the Diagnosis and Management of Individuals with Alpha-1 Antitrypsin Deficiency. Population: A Study of Data from the Third National Health and Nutrition Examination Survey. The Growing Burden of Chronic Obstructive Pulmonary Disease and Lung Cancer in Women: Examining Sex Differences in Cigarette Smoke Metabolism. Gene-Environment Interactions in the Development of Chronic Obstructive Pulmonary Disease. Worldwide Racial and Ethnic Distribution of 1-Antitrypsin Deficiency: Summary of an Analysis of Published Genetic Epidemiologic Surveys. National Hospital Discharge Survey, 1979-2004, 2005 unpublished data provided upon special request. Surprisingly High Prevalence of Anxiety and Depression in Chronic Breathing Disorders. Long-term Continuous Oxygen Treatment in Chronic Obstructive Pulmonary Disease: Proper Use, Benefits and Unresolved Issues. Lung-Volume Reduction Surgery for Pulmonary Emphysema: Improvement in Body Mass Index, Airflow Obstruction, Dyspnea, and Exercise Capacity Index After 1 Year. Long-term Follow-Up of Patients Receiving Lung-Volume-Reduction Surgery Versus Medical Therapy for Severe Emphysema by the National Emphysema Treatment Trial Research Group. Inhaled Corticosteroid Use in Chronic Obstructive Pulmonary Disease and the Risk of Hospitalization for Pneumonia. Inhaled Corticosteroids and Risk of Lung Cancer Among Patients with Chronic Obstructive Pulmonary Disease. Salmeterol and Fluticasone Propionate and Survival in Chronic Obstructive Pulmonary Disease. Economic Implications of Newborn Screening for Cystic Fibrosis: A Cost of Illness Retrospective Cohort Study. Neonatal Screening for Cystic Fibrosis Is Beneficial Even in the Context of Modern Treatment.
World Health Organization: Department of Child and Adolescent Health and Development erectile dysfunction protocol formula generic super p-force 160mg free shipping. Acute infection with hepatitis C is usually asymptomatic impotence nasal spray buy generic super p-force 160mg line, but 50%-60% of children and 60%-70% of adults will go on to erectile dysfunction names cheap 160mg super p-force overnight delivery develop chronic hepatitis erectile dysfunction young adults treatment cheap super p-force 160mg mastercard, of which many will progress to cirrhosis and primary hepatocellular carcinoma. Treatment should be started in patients with chronic hepatitis C progressing to cirrhosis. The two treatment regimens that are currently used are interferon alfa alone and interferon alfa in combination with ribavirin. Antiemetics for children with gastroenteritis: off-label but still on in clinical practice. Guidelines for the control of shigellosis, including epidemics due to Shigella dysenteriae 1. Management of severe malnutrition: a manual for physicians and other senior health workers. Discuss relevant laboratory findings in anemia, neutropenia, and thrombocytopenia. This chapter reviews normal hematopoiesis and the clinical manifestations of children with altered hematopoiesis, followed by a discussion of the causes of the different manifestations of altered hematopoiesis and their management and treatment. Normal Hematopoiesis To understand abnormal blood cell production, one must know how normal hematopoiesis occurs. In addition to the stem cell, supportive cells, called stromal cells, must be present for normal hematopoiesis to occur. This change affects all three cell lines (red blood cells, white blood cells, and platelets) that come from stem cells in the marrow. Erythropoietin, produced in the kidney, and thrombopoietin, produced in the liver, are necessary for proliferation and production of red blood cells and platelets, respectively. The progenitors of the red blood cells are in the erythroid lineage, whereas the white blood cells are derived from the granulocytemacrophage colonies of progenitor cells, and finally the megakaryocytes of the bone marrow give rise to circulating platelets. Alterations in hematopoiesis can lead to abnormalities in red cell, white cell, and platelet count in the peripheral blood. A decrease in the number of white cells is called leukopenia, and a decrease in the number of platelets is called thrombocytopenia. Anemia is further classified by the size of the red cells in the peripheral blood as microcytic (smaller than normal), normocytic (normal), or macrocytic (larger than normal). The most common changes seen in morphology of the marrow architecture include decreased cellularity and myelodysplasia (abnormal change of the cellular structure) affecting the cells of the erythroid lineage and the megakaryocytes. This development in turn leads to abnormal maturation of the different bone marrow cell lineages and may explain the preceding structural changes. This Clinical Manifestations of Altered Hematopoiesis Children with alterations in hematopoiesis should have a comprehensive patient history, physical examination, complete blood count, and liver function tests. A peripheral smear should be examined because it provides a great deal of information on cell morphology and can give clues to the cause of the alteration in hematopoiesis. The following sections review the signs and symptoms of anemia, neutropenia, and thrombocytopenia. Trimethoprim-sulfamethoxazole used to prevent and treat Pneumocystis jirovecii pneumonia also suppresses the bone marrow. One should consider the diagnosis of bone marrow dysfunction especially if there are decreases in more than one cell line. Many other factors can cause anemia, which when present alone is not as concerning for bone marrow suppression. Evaluating a child for marrow suppression requires bone marrow aspiration and biopsy, and the marrow should also be sent for mycobacterial stains and culture. Treatment of bone marrow suppression is predicated on therapy for the underlying cause. Anemia due to iron deficiency is microcytic, and that due to B12 deficiency has associated changes in the neutrophils known as megaloblastic change. Myelosuppressive drugs such as zidovudine and trimethoprim-sulfamethoxazole can also lead to anemia. The anemia associated with zidovudine treatment is macrocytic, and indeed the red cells may be macrocytic even without anemia. Finally, anemia can be a result of red cell destruction, or hemolysis, as opposed to an aberration of production.
References:
- http://unmhospitalist.pbworks.com/w/file/fetch/109795702/jrv160015.pdf
- https://www.accessdata.fda.gov/drugsatfda_docs/label/2009/022268lbl.pdf
- https://www.connecticutchildrens.org/wp-content/uploads/2019/03/Annual_Academic_Report_2018_LowRes.pdf
- https://foodinsight.org/wp-content/uploads/2011/08/Final-Functional-Foods-Backgrounder.pdf
- https://aristopharma.org/wp-content/uploads/2020/01/The-Scientific-Times-Vol-4-ADA-guidelines-2020.pdf



