
Benazepril
"10 mg benazepril free shipping, medications 7 rights."
By: Lars I. Eriksson, MD, PhD, FRCA
- Professor and Academic Chair, Department of Anaesthesiology and Intensive Care Medicine, Karolinska University Hospital, Solna, Stockholm, Sweden
The variability in cyst formation and disease severity depends on the locus affected and how much protein is being made symptoms 5 days past ovulation buy 10 mg benazepril with amex. These extrarenal problems include mitral valve prolapse symptoms of breast cancer proven 10 mg benazepril, hypertension medications metabolized by cyp2d6 buy 10 mg benazepril, extrarenal cysts treatment 12mm kidney stone buy 10 mg benazepril mastercard, aortic aneurysms, intracranial aneurysms, hernias, colonic diverticula, cholangiocarcinoma, and congenital hepatic fibrosis (4). Intracranial aneurysms are a significant cause of mortality when they rupture (4). As children age, the number and size of cysts increases and therefore, the sensitivity and specificity of diagnosis by ultrasound increases as children become older (4). Chronic renal insufficiency is monitored carefully, especially with respect to its effects on nutrition and growth (4). Hypertension is treated with antihypertensives and urinary tract infections are treated appropriately. Screening for intracranial aneurysms should be performed in teenagers with a family history of intracranial aneurysms due to the serious consequences of rupture (4,5). Potter syndrome is variably defined as including congenital renal failure or cystic kidneys associated with oligohydramnios, abnormal facies and hypoplastic lungs. Potter syndrome is generally incompatible with life due to congenital renal failure and pulmonary hypoplasia. There can also be signs of respiratory distress or abnormal feeding due to the compressive effects of enlarged kidneys. A biopsy of her kidney at that time revealed a diffuse proliferative glomerulonephritis with prominent crescents and minimal fibrosis. An echocardiogram reveals a moderate pericardial effusion, but is otherwise normal. This may include nausea and vomiting, altered mental status, seizures, pericarditis or bleeding diathesis (platelets become progressively dysfunctional in the setting of uremia). As with any central venous line, there is a risk of pneumothorax if the internal jugular or subclavian sites are used; a risk of bleeding (especially in the uremic patient) and a risk of infection. If kept in for an extended period, infection is one of the drawbacks to having this type of vascular access; however, it can be used immediately and is ideal when dialysis needs to be done quickly. If chronic, "maintenance" dialysis is planned for some future time (as with chronic renal failure), more permanent vascular access should be established. It is usually done in the non-dominant arm, in case ischemia or other complications occur. Once it is decided that permanent vascular access is needed, the patient and nurses should be instructed to make that limb "off-limits" for blood draws, intravenous lines or arterial punctures. This is done to minimize any potential trauma to the blood vessels prior to fistula surgery. This includes edema or ischemia of the hand, pseudoaneurysm at the graft or fistula site, infection, thrombosis and congestive heart failure. Once vascular access is established, blood leaves the body via tubing into the dialysis unit. It passes along a semipermeable membrane with a dialysis solution (dialysate) flowing along the other side of the membrane. Solute particles from the blood then pass down their concentration gradient into the dialysate for removal. The mechanism of dialysis can be simplified based on standard diffusion: where particles (solutes) of high concentration (in the blood) move down their concentration gradient to an area of low concentration (the dialysate). Other aspects of the dialysis prescription include the type of membrane, flow rate of blood and dialysate, temperature, length of time on dialysis, and composition of the dialysate. Modern machines can monitor these functions and monitor for potential air emboli and blood leaks in the dialyzer as well. If the same patient had a viral gastroenteritis and her pre-dialysis potassium was 3. When patients are unable to tolerate such a drop in blood pressure or are already on vasopressor support (for example, in septic shock) another form of dialysis may be required. It is used almost exclusively in the intensive care unit for critically ill patients.
Deficiencies of glucocorticoids and mineralocorticoids result in the opposite conditions symptoms miscarriage cheap 10 mg benazepril with amex. Adrenal disorders result when the production of any of these hormones is insufficient or in excess symptoms ruptured ovarian cyst generic benazepril 10 mg with amex. The second type of adrenal Page - 522 insufficiency in pediatrics is acquired medicine to stop diarrhea purchase benazepril 10mg mastercard, typically idiopathic and presents during childhood and adolescence (see second case above) medicine runny nose buy 10mg benazepril with mastercard. Although the exact pathophysiology for the lack of a normal aldosterone effect is still debatable, the resulting saltwasting abnormalities can lead to severe life-threatening hyperkalemia, hyponatremia and acidosis. Approximately two-thirds of children with classical 21-hydroxylase deficiency will present clinically with the salt-losing form within the first 2 to 3 weeks of life. A rare condition that may mimic salt-losing congenital adrenal hyperplasia, and which must be considered in the differential diagnosis is pseudohypoaldosteronism. The usual infant with the salt-losing form of congenital adrenal hyperplasia will present with dehydration and signs of both acute and chronic hypovolemia, with or without peripheral vascular collapse, sometime between the third and 28th day of life. Such signs, however, may appear under uncommon circumstances as late as three to four months of age. More recent studies based on newborn screening data, however, have revealed more predictable gender proportions, thus supporting the value-added benefits of such a prevention strategy of newborn screening for treatable metabolic defects. Patients with the salt-wasting form will additionally demonstrate laboratory evidence of hyponatremia and hyperkalemia in association with a suppressed aldosterone concentration and an elevated plasma renin activity. A simple test to demonstrate inappropriate salt wasting from aldosterone deficiency is to obtain a urine sodium measurement when the patient is hyponatremic. In contrast to the expected findings of appropriately low urine sodium in the setting of hyponatremia, the urine sodium in salt wasting states such as mineralocorticoid deficiency or resistance will be inappropriately high. Both finger and toe nails can be affected with findings of opaque, thickened, friable and brittle nails. Given the widespread use of corticosteroids as therapeutic anti-inflammatory agents in the treatment of such conditions as asthma, arthritis or as adjunctive chemotherapy, iatrogenic adrenal insufficiency is at present, probably the number one etiology of adrenal cortisol deficiency. Supraphysiologic dosages of exogenous corticosteroids for periods as short as 4 weeks have been associated with the prolonged (up to one year! For glucocorticoid replacement, an initial bolus of glucocorticoids, such as hydrocortisone sodium succinate, or its therapeutic equivalent (See table 1), must be administered intravenously at a bolus dose of 60 to 80 mg per square meter (body surface area). As soon as a pattern of clinical improvement has been established, one-third to one-half of the initial dose of intravenous hydrocortisone sodium succinate must be continued every 4 hours for the subsequent 24 hours, by which time effective glucocorticoid replacement should be complete. Unfortunately, although Florinef is an effective medication for long-term maintenance therapy, the acute biochemical mineralocorticoid effects of oral fludrocortisone acetate may be delayed by 48 to 72 hours. Until then, the continued infusion of salt containing intravenous solutions will be needed to correct the hyponatremia and hyperkalemia seen with salt-losing adrenal insufficiency. Using hourly bedside monitoring, blood sugar levels below 60 mg/dl should be avoided and treated with intravenous dextrose as indicated. When signs of hyperkalemic electrocardiographic toxicity exist, the patient must be treated aggressively to avoid clinical toxicity. Although parenteral calcium is potentially effective in converting the dysrhythmia to a perfusing sinus rhythm, hyperkalemic dysrhythmias will recur unless the serum potassium level can be reduced. Other rapid measures for treating severe hyperkalemia by similarly shifting potassium intracellularly include: 1) albuterol aerosol and 2) insulin (0. These latter potassium-lowering methods are only temporary since they merely shift potassium intracellularly. Intravenous fluids containing a sodium chloride solution with dextrose should be continued until the institution and tolerance of oral feedings allows for adequate sodium intake. Suppressed plasma renin may alternatively suggest an excess mineralocorticoid effect especially in the presence of an elevated blood pressure. Adrenal disorders localized to the adrenal medulla are even more rare, especially in pediatrics. The presenting clinical symptoms are directly related to the excess catecholamines released by these tumors. The diagnosis may thus be difficult to establish and may require multiple investigations. Treatment is directed at surgical removal of the primary tumor with pre-operative, medical stabilization of the associated hypertension. Neuroblastomas, ganglioneuromas and ganglioneuroblastomas are additional tumors of the adrenal medulla.
Glucocorticoids medicine lodge kansas discount benazepril 10 mg without prescription, diuretics medicine emoji purchase 10 mg benazepril with visa, demeclocycline medicine daughter lyrics buy 10mg benazepril mastercard, lithium medications information purchase 10 mg benazepril amex, foscarnet, and methicillin may all cause nephrogenic diabetes insipidus (2). The pathophysiology that underlies central, gestational, and nephrogenic diabetes insipidus are similar. It is thought that this may be the result of washout of the medullary concentration gradient or inhibition of aquaporin-2 synthesis. The hallmarks of diabetes insipidus are polyuria (2-20 liters per day) and increased fluid intake (3). Polyuria is always accompanied by a proportionate polydipsia that is usually, but not always, attributable to increased thirst (2). However, dehydration and hypernatremia may be present especially after hypothalamic damage secondary to shock or anoxia (3). The diagnosis is made mainly on clinical grounds with some laboratory supportive evidence. However, hyperuricemia implicates central diabetes insipidus as decreased V1 stimulation decreases urate clearance. The expense and inconvenience of this treatment, however, make this regimen impractical. Symptomatic hyponatremia has a mortality of 10 to 15%, and the mortality rate is higher when the serum sodium level is below 110 mEq/L (4). Acute water retention causes neurologic symptoms by rapidly increasing the intracellular volumes of brain cells and thus inducing cerebral edema. This can cause permanent neurologic damage, for example central pontine myelinolysis and death (4). The proximity of the genes for vasopressin and oxytoxin, less than 12kb within the human genome, is thought to explain this phenomenon as a single transcription factor could activate both promoters (4). Water retention leads to expansion of both the extra and intracellular compartments. The rate at which these abnormalities develop varies widely depending on the magnitude of the imbalance between the total rate of water intake and excretion by renal and extrarenal routes. On the other hand, if urinary concentration is fixed at a high level and insensible loss is low, even an apparently normal basal rate of fluid intake may be sufficient to produce the syndrome (2). This is abnormal since the urine should be very dilute if the plasma is hypo-osmolar. Checking the serum and urine sodium levels are often sufficient since hyponatremia in conjunction with an elevated urine sodium is similarly abnormal, although this can also be caused by diuretics, mineralocorticoid deficiency (Addisonian crisis) and salt losing nephropathy. The most striking and potentially confusing variant is that caused by downward resetting of the osmostat. If the measurements of urine osmolality are repeated during therapeutic fluid restriction, the true cause becomes apparent because urinary concentration begins long before serum sodium rises to normal. These distinctions can usually be made on the basis of the clinical history, physical examination, and routine laboratory tests. Because of this effective hypovolemia, plasma urea, uric acid, renin activity, and aldosterone are also usually elevated, and the urinary excretion of salt and water is decreased. The resultant depletion of intravascular and interstitial fluid results in physical signs of hypovolemia, such as tachycardia and postural hypotension. Consequently, plasma urea, uric acid, renin activity, and aldosterone are elevated, whereas urinary excretion of salt and water are reduced (unless a diuretic or sodium-losing nephropathy is responsible). In others, it is an acute self-limited disorder that remits spontaneously within 2 to 3 weeks. If the hyponatremia is severe, or accompanied by symptoms such as nausea, vomiting, coma, or seizures, it may be desirable to correct part of it more rapidly by combining fluid restriction with a slow intravenous infusion of hypertonic (3%) saline. Besides polyuria and polydipsia, physical exam and lab studies are typically within normal limits. However, in severe cases, signs and symptoms of hypernatremia and dehydration may be present. Vasopressin challenge test: polyuria and polydipsia are corrected in central diabetes insipidus, but not corrected with standard doses in nephrogenic diabetes insipidus. There are 4 types, only one is regulated by osmolality; however, the osmostat is reset to a lower osmolality. If the urine sodium is low, then the hyponatremia is due to total body sodium depletion. Her parents report that she cries when touched in her hands and feet and has refused to walk.

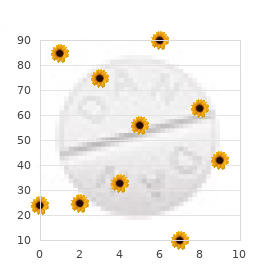
New data and analyses have reduced sampling uncertainty symptoms 7 days post iui discount 10mg benazepril with amex, but uncertainties related to symptoms bipolar buy 10 mg benazepril mastercard estimating risk for exposure at low doses and dose rates and to treatment glaucoma order benazepril 10 mg free shipping transporting risks from Japanese A-bomb survivors to 7r medications purchase benazepril 10mg fast delivery the U. Plotted points are estimated excess relative risks of solid cancer incidence (averaged over sex and standardized to represent individuals exposed at age 30 who have attained age 60) for atomic bomb survivors, with doses in each of 10 dose intervals, plotted above the midpoints of the dose intervals. Solid and dotted lines are estimated linear and linear-quadratic models for excess relative risk, estimated from all subjects with doses in the range 0 to 1. A linear-quadratic model will always fit the data better than a linear model, since the linear model is a restricted special case with the quadratic coefficient equal to zero. For solid cancer incidence however, there is no statistically significant improvement in fit due to the quadratic term. It should also be noted that in the low-dose range of interest, the difference between the estimated linear and linear-quadratic models is small relative to the 95% confidence intervals. The insert shows the fit of a linear-quadratic model for leukemia to illustrate the greater degree of curvature observed for that cancer. Research Need 3: Evaluation of the relevance of adaptation, low-dose hypersensitivity, bystander effect, hormesis, and genomic instability for radiation carcinogenesis Mechanistic data are needed to establish the relevance of these processes to low-dose radiation exposure. Relevant end points should include not only chromosomal aberrations and mutations but also genomic instability and induction of cancer. In vitro and in vivo data are needed for delivery of low doses over several weeks or Copyright National Academy of Sciences. Research Need 9: Future occupational radiation studies Studies of occupational radiation exposures, in particular among nuclear industry workers, including nuclear power plant workers, are well suited for direct assessment of the carcinogenic effects of long-term, low-level radiation exposure in humans. Ideally, studies of occupational radiation should be prospective in nature and rely on individual realtime estimates of radiation doses. Where possible, national registries of radiation exposure of workers should be established and updated as additional radiation exposure is accumulated and as workers change employers. These registries should include at least annual estimates of whole-body radiation dose from external photon exposure. These exposure registries should be linked with mortality registries and, where they exist, national tumor (and other disease) registries. It is also important to continue follow-up of workers exposed to relatively high doses, that is, workers at the Mayak nuclear facility and workers involved in the Chernobyl cleanup. Research Need 10: Future environmental radiation studies In general, additional ecological studies of persons exposed to low levels of radiation from environmental sources are not recommended. However, if there are disasters in which a local population is exposed to unusually high levels of radiation, it is important that there be a rapid response not only for the prevention of further exposure but also for scientific evaluation of possible effects of the exposure. The data collected should include basic demographic information on individuals, estimates of acute and possible continuing exposure, the nature of the ionizing radiation, and the means of following these individuals for many years. The possibility of enrolling a comparable nonexposed population should be considered. Studies of persons exposed environmentally as a result of the Chernobyl disaster or as a re- months at very low dose rates or with fractionated exposures. Research Need 4: Identification of molecular mechanisms for postulated hormetic effects at low doses Definitive experiments that identify molecular mechanisms are necessary to establish whether hormetic effects exist for radiation-induced carcinogenesis. Research Need 5: Tumorigenic mechanisms Further cytogenetic and molecular genetic studies are necessary to reduce current uncertainties about the specific role of radiation in multistage radiation tumorigenesis. Research Need 6: Genetic factors in radiation cancer risk Further work is needed in humans and mice on gene mutations and functional polymorphisms that influence radiation response and cancer risk. In humans, the problem can be explored using genomic databases and knowledge of mechanisms of origin of radiation-induced deletions to predict regions that may be particularly prone to radiationinducible deletions. With respect to epidemiology, studies on the genetic effects of radiotherapy for childhood cancer should be encouraged, especially when they can be coupled with modern molecular techniques (such as array-based comparative genomic hybridization). Research Need 8: Future medical radiation studies Most studies of medical radiation should rely on exposure information collected prospectively, including cohort studies as well as nested case-control studies. Future studies should continue to include individual dose estimation for the site of interest, as well as an evaluation of the uncertainty in dose estimation. Studies of populations with high- and moderate-dose medical exposures are particularly important for the study of modifiers of radiation risks. Because of the high level of radiation exposure in these populations, they are also ideally suited to study the effects of gene-radiation interactions, which may render particular subsets of the population more sensitive to radiation-induced cancer. It is important that follow-up for mortality and cancer incidence continue for the 45% of the cohort who remained alive at the end of 2000.
Generic benazepril 10mg amex. 14 months off benzo withdrawal symptoms.
References:
- https://www.who.int/docs/default-source/wpro---documents/emergency/surveillance/dengue/dengue-20201105.pdf?sfvrsn=fc80101d_42
- https://link.springer.com/content/pdf/10.1007%2F978-1-4612-6060-8.pdf
- https://www.metlife.com/content/dam/metlifecom/us/homepage/stateofks/pdf/State_of_KS_CII_Plan_Summary.pdf
- https://www.ecronicon.com/ecmi/pdf/ECMI-15-00745.pdf
- https://www.tn.gov/content/dam/tn/health/program-areas/lab/directory-of-services/nbs/3_Methyl_Crotonyl_CoA_Carboxylase_Deficiency_rev_8.20.pdf



